All of this information is contained in the USMLE GUIDE.doc so that you can take it with you and not worry about your internet connection. I post all of it here for those that do not have Microsoft Word and so that people can find it through search engines. Hope it helps.

A word on this guide:
I just finished my second year at St. George’s University School of Medicine. Figuring out what you are going to do for the Boards is a pain in the ass and gets people nervous that they do not have a plan. Many of them sign on to Kaplan or Falcon for this reason. I would like to prevent as many people as possible from signing up for those courses for those reasons, as they are expensive and you are poor. I want you to have a plan, an idea of what to expect, and all of that free. I hope this helps.
A word on advice:
I am wary of most advice. It is often unqualified, and by this I mean that I do not know why I should believe in your expertise. Did you score well and are you willing to tell me the score behind this advice? Are you like me in that we learn, memorize, and study alike? What works for Peter may fail for Paul and it is good to keep this in the back of your mind as everyone begins to tell you what you should and should not do. The other problem that I have with a lot of advice is that I am not told the reason behind the conclusion. It is easy to say, “Just do questions”, but it is much harder to give a well thought out argument to support your advice. There may be an excellent reason, but many people do not think to ask for it or to give it. Also, it takes a fair bit of time.
If someone says that there is a lot of Embryo on the test, please kick him in the face. That sort of advice (even if it ends up being true) is worthless for planning. The most frustrating part of this whole experience is that n=1 and it is hard to draw conclusions from a sample size that small. You will wonder if you did it correctly, how you would have scored if you changed blah blah, and so on. That leads us to why I am writing this:
Medical school is great because it is the end of decisions. Decide to go to medical school. Three and a half years later: decide what kind of doctor to be. Three to five years later: decide which job to take. That is three decisions over ten years and medicine is great that way. I was so tired of making decision about how to study that I wished someone had done it all for me. This guide is meant to be a turn-off-your-brain and do-as-I-say outline so that you can save yourself from all of that. It is the guide that I wish someone had made for me.
A word on irony:
I am aware of the irony that I am writing a little guide filled with advice while not offering my score, telling you about myself, etc. What I can give is my reasons for each decision so that even if you do not end up following it, you at least see the problem of planning and studying as manageable. If you are interested, when I get my score I will post it and at that point, you can decide to continue using this guide or decide to forget everything written here. Deal? Now on with the show…
THE SCHEDULE
I am assuming that you are taking six weeks to study for this test. If it is shorter or longer, I have structured this so that it is easy to change according to your unique schedule. This schedule is built using the newest edition of the First Aid for the USMLE Step 1 (Systems based) as I think it is the best game in town and damn near everyone seems to own it. We need a calendar, and we need to divide it into two main sections: cramming and pre-cramming.
CRAMMING
Cramming is undervalued. I took an incredibly long time to prepare (9 weeks) so that I would not have to cram because (cue lame music) I wanted to really understand the material. Fair enough, but the last two weeks are for cramming. You can realistically cover two topics each day. Anything more and you are skimming. I have good reasons for each of these choices, but first you should just take a look at what we will call “the cramming”.

The day before the test, you will be tired of studying (more so). This is when you are most vulnerable to total mental collapse. A friend described it to me: “I opened up Micro to look over viruses once more before the test and I realized that I had forgotten how to read. It was as if my head had exploded onto the table and I could not pick it back up again. I postponed the test a week after that.” To avoid this, I advocate taking a half-day and seeing a movie. It was one of the few things that I did that worked.
Before you start this final sprint, take a day off. You have earned it. I think you should begin with Biochemistry because the meat of this subject is in the underpinnings of other diseases. A good look in the beginning will help you interpret things later on and will reinforce the pathways that actually matter. By putting this first, you effectively study it all week. It is a big topic, so it gets two days. Molecular genetics and Immuno cover some similar ground (signaling) and this is a nice lead in to Micro. I will make the same argument about Micro, that putting it this early means that you study it with every system to come, reinforcing the pathogens. It is big, so also earns two days.
Cardio and Heme/Onc are thrown together because of the pathology. For similar reasons, I have placed them next to Musculoskeletal. As you will find, the vasculitides are covered in Musculo, not in Cardio or Heme/Onc, so these three topics are overlapping in the First Aid which is why I have grouped them. Cardio, Heme/Onc, Gastro, and Musculo are also grouped because chances are that one of these topics is a strength for you, so going through that subject quickly allows a weakness in the others to expand into that day.
Neurology and Psychiatry are next to each other for the association. Neuro, unfortunately, is just too big to group with a second large topic, so this is as good a place as any to split up Behavioral with Psych (they pair naturally) and Biostats with Neuro. Renal and Respiratory are not as big as the other sections and this should make for a somewhat easier day. These are grouped together in hopes that you finally sit down and learn Acid/Base compensation. After two years, it is time.
Embryology is tricky. Most of it belongs with Reproduction and Endocrine while the rest is spread out among all the systems. The best advice I have is that you study the Embryology for each system in the morning before getting into the thick of each subject and save the Repro/Endocrine stuff for the end. That it is a hodgepodge also makes it a natural move to group it with Basic Pharmacology and Basic Pathology. These sections are short and represent a little bit of everything. If you give it a good read, it can pull topics from earlier in the week together and is not too stressful to be studying up to test day.
And with that, use the last day before the test to print out your permit, print out the directions to your testing center, and look over some topics that you had to skip. Try to force yourself to stop studying by midday and do something non-medical that night like watching a new movie with a friend. The night before my test I caught 300, and it was great to think about something other than pathways for at least those two hours.
PRE-CRAMMING
That was cramming. Now, onto pre-cramming. Since we have six weeks and I just stole the last two weeks for cramming, that gives us exactly 30 days to prepare. Remember that you are not preparing for the test during this period; you are preparing for “the cramming”. If you do not cover everything in a section in the time allotted, it will not be the end of the world. You will get another crack at it, at which point not getting to it will be the end of the world. Ready for the suck? Seriously, stay optimistic.
If you are a numbers person, we have 30 days to cover 329 pages of the First Aid, which works out nicely to 11 pages a day. This is a lazy way to weight things, but who cares? I have gone to the trouble of counting each page per section for you, and arranged the following. Here is the first two weeks.

We start out with something general and familiar: the basics. Most of the connections in this section went over my head and I did not pull them together until the end, but it is nice to have the early exposure and to ease into this whole thing before the real subjects start. This brings us to Biochemistry. It is big and intimidating for a lot of students and three days does not seem like enough, but it has to be just three days. First, we give it two full days in the last two weeks of cramming. Second, the other subjects need to be given time and are likely higher-yield.
It does not let up as Biochemistry feeds into Immunology and Microbiology. Again, three days is not enough to cover Microbiology, but the other subjects need to be covered and we give Micro two full days during cram week. Behavioral science and Biostatistics are meant to be your first break. The ground of Behavioral science will be touched again during Psych, and Biostatistics is not that big. You can either take half the day off or use the extra time on Micro. As always, make sure you are not seeing anything for the first time during “the cramming”.
Embryology is just not big enough to get its own day and should be learned in pieces with each system that follows. What is important for now is the developmental aspect. You can combine it with the first day of Endocrine (as I have done) or group it with Reproduction, does not really matter so long as you get to it. I think these three topics together makes each of them stronger, and this might be the first time you really understand the menstrual cycle.

The second two weeks begin the systems. I was taught subject-based, but for the type of thinking that makes for good test scores, the integration that comes with doing Anatomy, Physiology, Pathology, and Pharmacology together just cannot be beat. If your school taught this way then this is old hat for you, but for me it was a shock to see all the new connections.
We begin with the Cardio/Heme/Onc/Musculoskeletal combination for the reason I described earlier. Cardio looks big in the First Aid and the pharmacology of Heme/Onc can be intimidating. Just remember that “screw it, I’m just not going to know that” is a perfectly good assessment for some of the material and if you can make peace with that, you will be less stressed. It probably will not be on your test anyway. Or you fly through these sections and earn a day off.
Gastrointestinal is there because where else would you put it? Renal and Respiratory go together with their acids and bases, and this brings us to the skull. Psychiatry is a new section with the First Aid and I think they have done a good job. It may bleed over into Neuro (as far as BRS and other review books go) but the two of them together get four days now and two more days during “the cramming”.
All together now:
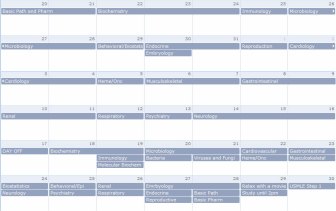
If you are taking less time or more time, you simply shave or add a day here and there from one of the blocks in the first four weeks. I do not think it is a good idea to steal or add days from “the cramming” as this is a period favored by the gods. Why not add? “The cramming” is the period where you realize that everything you are reading is the last time you will get to see it before the test, and this is a shocker if you have not prepared for it. Cramming is also useful in the short term, and once you extend that period past two weeks, I think it is a hard argument that your short-term memory is still holding onto the lessons in the first days. Just my advice, but then again I could have done poorly and you should ignore all of this. You can access this calendar online. The dates used are from May 20th, 2007 – June 30th.
QUESTIONS
Which QBank is the best? USMLE WORLD. But that would be shitty advice, right? I could just cut and past the whole thing here, but I would like to keep this file manageable. Please read my evaluation of free questions and Qbanks available online.
BOOKS
Everyone is chasing after that magic bullet: the high-yield book. My experience was that few books can pull this off well and that most try to be miniature textbooks and are unmanageable in the time you have (HY Cell and Molecular by Dudek, HY Neuroanatomy by Fix) or are bare bones and do not help you make many connections (BRS Path). After spending a good chunk of change on these review books, I should have just covered the material in the First Aid using my own textbooks. Most of what you read you will not have to look up (because you learned it) and the things you do look up will be surrounded with full explanations. Anything less than a full answer is annoying and wastes time (if, like me, you tend to dwell). If you have played it correctly, you should also have old review notes from your courses and it is always easier to remember what you used to know instead of starting from scratch with everything. By the end, I was using Golan’s Principles of Pharmacology, Robbins’ Basic Pathology, and the Merck Manual. The Pathology BRS by Schneider and Szanto was useful as an outline (which I used to focus on Robbins) but the questions for each chapter are absolute crap. Costanza’s Physiology BRS was good in parts and her questions were reasonable, but there are a few uncovered topics.

FIRST AID
I tip my hat to Graham Azon of Over!My!Med!Body! for this piece of advice: put the First Aid in a binder. I took my copy to an Office Max, had the spine cut off and the book three-hole-punched, and put it into a 1.5” binder. Best move I ever made. I was able to take separate notes and include them exactly where I needed them and I was able to take my notes from previous courses and include them (my roommate expanded the book to fill two 1.5” binders). It is hard to overstate the advantage of having everything you need in one place.
THE EXAM ITSELF
It is hard to anticipate the pace of this test. When doing timed questions in preparation, there were instances where I would finish with 10 or 20 minutes left. I thought to myself, “Self, you’re going to have plenty of time to look over questions in each block”. I was wrong. On test day, I had around 10 questions marked per block that I wanted to give a second look and two minutes to do it. It was unexpected and unsettling, and for this reason I wished that I had taken the NBME practice test at the center. It is worth it just to remove the final few unknowns for test day.
The clock counts down for each block while you move up the list of questions. Unless you are willing to do the calculation (even subtraction can be stressful), it is hard to know how fast you need to move to finish. For pacing purposes, I ended up starting each block with question #50 and ending with #1. This way I knew exactly how many extra minutes I had to devote to problems as I went along and it helped me gauge whether I had to come up with an answer now (because I was falling behind) or could mark it for later (since I had a seven minute cushion). I would do this again.
I am thankful for the advice I received from a stranger: “You are going to walk out of the test with incredible relief that it is over. This will be mixed with some despair since you will think that you failed. It is over. You did not fail. Everyone feels that way.” He was right, and every one of my friends has echoed it. I went from relief, to defeat, to anger that I had not done better. A week later, I feel “okay”. When you go through it, remember that you are not the first, not the last, and it is normal.
Hope it helps, topher.



 Posted by rumorsweretrue
Posted by rumorsweretrue 









